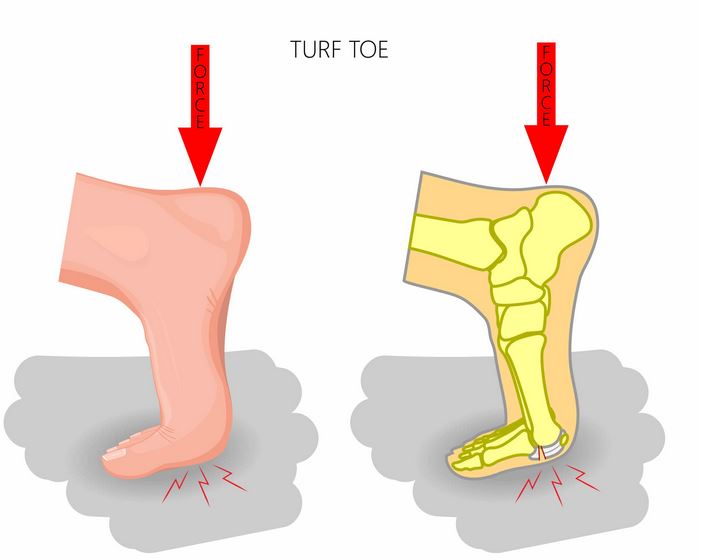
Turf toe is an acute injury to the first metatarsophalangeal joint. It is more likely in field sports associated with ‘turf’ playing surfaces, especially the artificial surfaces, hence the name ‘turf toe’. The problem is one of a sprain of plantar capsule of the joint and an impact injury to articular cartilage in the joint. Turf toe is commonly due to hyperextension of joint with the foot in a slightly dorsiflexed position (see image above) which can often occur in a tackling situation in foot ball sports.
Cause of Turf Toe
The typical mechanism of injury is due to hyperextension with axial loading of first metatarsophalangeal joint when the forefoot is fixed to the ground.

Symptoms of Turf Toe
The immediate acute symptoms of turf toe include pain, swelling, bruising and limited range of motion at the base of the big toe. The pain is worse with movement and weight-bearing activities
The diagnosis is typically based on a physical examination, assessment of the symptoms and identifying the mechanism by which the injury occurred. Imaging by X-rays or MRI scans may be used to rule out other potential causes and or to evaluate the extent of the ligament damage from the injury.
Grading of Turf Toe
- Grade I: sprain of the plantar plate.
- Grade II: partial tear of the plantar plate.
- Grade III: complete tear of the plantar plate
Treatment of Turf Toe
The treatment of turf toe will depend on the extent of the tissue damage (grading).
- Initial: rest, ice, anti-inflammatory medication
- Immobilization: the extent and duration of this will depend on the amount of tissue damage. If very minor (Grade 1), a stiff soled shoe, perhaps with a rocker and carbon fiber plate inset may be all that is needed – the purpose here is to prevent or limit how much dorsiflexion occurs at the joint. If more severe (Grade 2), a walking boot or short leg cast may be needed for 2-6 weeks to provide more immobilization.
- As it improves: when the injury is stable, progressive movement with a gradual return to activity. Strapping may be needed to protect the joint during the early stages of the return to activity. A stiffer soled shoe with a rigid carbon fiber insert may be needed in the medium to long term.
- If its not improving: Cortisone injections may be tried. 1-2% may need a surgical intervention if the initial injury was severe (Grade 3) or the injury is not responding to the conservative approaches..
Forum discussions on Turf Toe
Managing turf-toe in football players
Severe injury – Plantar plate tear (big toe), FIVE months!
Personal Opinion on Turf Toe Injuries
I have not seen many acute turf toe injuries. Most of the turf toe problems that I have seen are those still having symptoms months and sometimes years after the initial injury. Generally, the initial management of the acute problem was possibly not as good as it should have been or the return to sport was done too quickly. Most of these do seem to respond reasonably well to mobilizations and manipulation of the first metatarsophalangeal joint and better use of the rigid carbon plate or stiff soles shoes with a rocker to limit motion during sport. Exercises that involve a lot of movement and load on the first MPJ can help (eg hopping; zig-zag or change of direction drills; etc). Those still playing sport at a reasonably higher level will probably need strapping to also help restrict motion of the joint during the more intense training activities and during competition.
Author:
University lecturer, runner, cynic, researcher, skeptic, forum admin, woo basher, clinician, rabble-rouser, blogger, dad.


